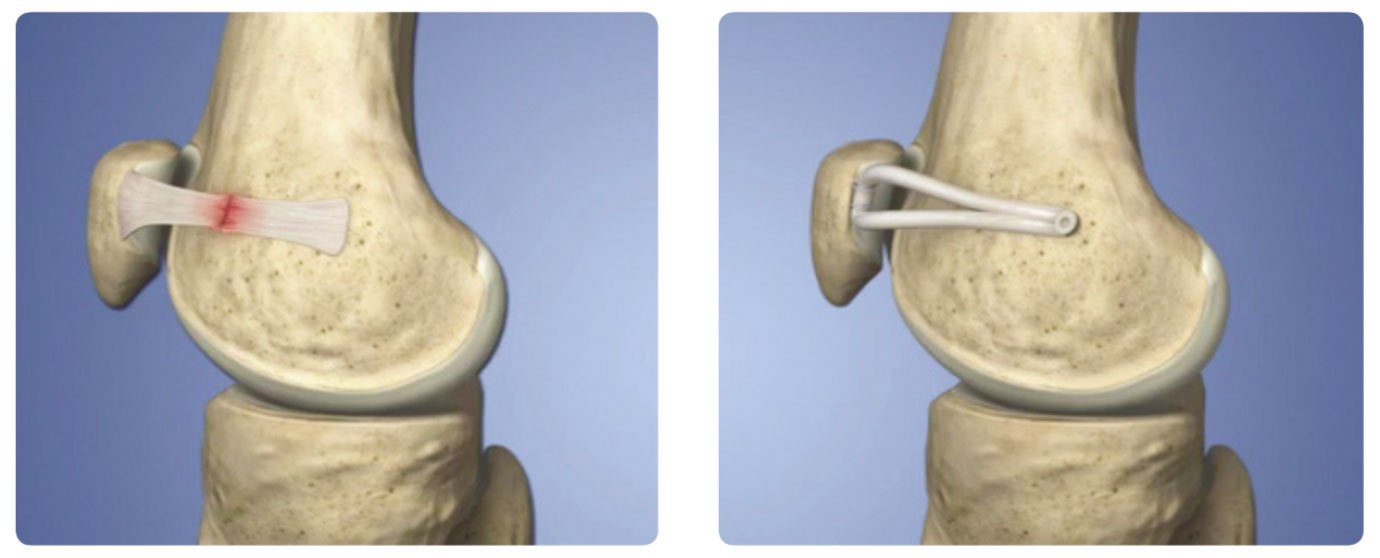
As you are aware, kneecap instability is problematic, and in your situation, I have recommended a ligament reconstruction to help stabilise the joint. This procedure is called a Medial PatelloFemoral Ligament (MPFL) reconstruction. The procedure is minimally invasive, meaning smaller incisions, less scarring and less post-operative pain. Minimally invasive procedures also facilitate early rehabilitation and a faster recovery.
The surgery involves taking a graft from one of your hamstring tendons (gracilis tendon) and using it to reattach the inside of your kneecap (patella) and thigh bone (femur). The graft bridging the two bones helps to to prevent the knee cap from dislocating to the outside of the knee again.
MPFL Reconstruction: Day of Surgery
You will be admitted to hospital on the day of surgery. My assistant will provide you with your admission time and fasting instructions prior to your arrival.
MPFL Reconstruction: Post-Operative Care
Inpatient Stay
Most patients are discharged from hospital after an overnight stay. We place your knee in a brace at the completion of surgery, and the staff at the hospital will help to show you how to put it on and take it off as needed.
Brace
Brace usually stays on at all times (including sleeping) for at least two weeks, aside from times where you are practicing ‘range of motion’ exercises.
Crutches
Crutches are used when mobilising for a variable amount of time. You can progressively increase the amount of weight you put through your operated leg as your comfort allows.
Range of motion
Knee stiffness does not tend to be a problem after this procedure, although It is advisable to perform some light bending and straightening exercises 3-5 times a day.
Ice, elevation and compression
Aim to elevate your knee (above the level of your heart) frequently, and ice your knee every two hours in the initial few days after surgery. You will have a compression bandage placed on your knee after surgery to help with swelling – this can be removed as necessary for icing.
MPFL Reconstruction: Wound Care
If the dressings remain dry there is no need to replace them, and at the two-week post-operative check I will remove them and check your wounds. If a dressing does become wet or need replacing, simply remove it and replace with a new one.
MPFL Reconstruction: Pain Relief
Regular paracetamol and anti-inflammatory medication (if indicated) are the primary sources of pain relief post-operatively. You will be given some stronger medications which can be helpful in the early post-operative phase.
MPFL Reconstruction: Follow Up
I will review you in the rooms approximately two weeks after surgery. If you are unsure of your follow-up appointment, please call my assistant on 9959135963 to confirm.
2-6 weeks
Ice the knee regularly and elevate the leg to help reduce swelling. Aim to re-establish a normal walking cycle. Physiotherapy during this phase is helpful to restore muscle and joint function. Once your knee feels stable you can start to walk short distances without the brace. You can commence some light swimming with a pool buoy between your legs and gentle stationary bike riding can be started.
6-12 weeks
During this phase you will work on building your thigh muscle strength, joint stability and confidence in the knee.
3 months plus
Exercises will increase in intensity at this time.
MPFL Reconstruction: Return to Sport
Each sport is specific, and we will discuss your expected return to play prior to surgery. In general, I aim for return to full participation in sports between 3 and 6 months.
MPFL Reconstruction: Driving
You can return to driving when you are walking comfortably unaided and have regained good control of your knee. In general this is a minimum of two weeks.
MPFL Reconstruction: Return to Work
I would advise taking at least the first two weeks after surgery off so you can rest, elevate your leg and get comfortable. For those doing heavy work, return to work can take between 6 and 12+ weeks, depending on the nature of work.
MPFL Reconstruction: Problems
Donor site pain
Discomfort at the back of the thigh where the hamstring tendon was harvested is common and will generally settle in the first 2-4 weeks.
Superficial Infection
Superficial Infection is not very common but can occur. It usually presents as redness and increased pain around the wound, and generally resolves with a short course of antibiotics.
Deep infection
Deep infection is rare and requires admission to hospital. Surgical ‘washing out’ out of the knee and high dose antibiotics administered intravenously are commenced as soon as possible.
Knee joint infection usually presents between 5 and 10 days post-operatively, with increased, increased swelling and a marked decrease in your range of movement.
If you are concerned about an infection, please contact me as soon as possible. During business hours the best point of contact is via my assistant .After hours, please contact the hospital where you had your surgery, and ask them to get in touch with me. Failing this, present to your local Emergency Department for review.
Numbness
Numbness may be experienced in the days following surgery. The risk of long-lasting numbness is very low with this surgery.
Foot and Ankle Swelling
Foot and Ankle Swelling may occur post-operatively. It generally reflects the effects of gravity on the swelling around your knee. If you have severe foot and ankle swelling, remove your compression bandage, elevate your leg above your body and ice your knee.
Re-Injury
Re-Injury is unusual in the early post-operative period. However, accidents happen, and if you are concerned your knee should be checked. Please contact the rooms if you have any concerns and we can organise a review.